


THE IMPORTANCE OF INFORMATION RECORDING IN TUBERCULOSIS CONTROL
Abstract
In order to analyze the quality of record keeping in the implementation of the Tuberculosis Control Policy was carried out a retrospective descriptive study of 863 medical records of patients seen at the CRA in the city of Serra, ES, 2004 to 2009.
Keywords
Tuberculosis; Epidemiological Surveillance; Disease Prevention
Introduction
Tuberculosis (TB) is still a serious public health issue which involves social, political and economic aspects. In 1993, the World Health Organization (WHO) declared TB state of emergency. Worldwide, people die more due TB than they do because of any treatable infection. TB affects more than 20.000 people a day and 5.000 die with its aggravation; one third of the world’s population is infected. There are 9.2 million patients per year, 80% of the cases are concentrated in 22 countries; 1.7 million deaths are annually recorded; 200.000 cases are associated with HIV; there are 500.000 cases caused by multidrug-resistance [1]. Brazil along with other 21 peripheral capital countries host 80% of the world cases [2.3].[1]
The guidelines of the National Tuberculosis Control Program (NTCP) coordinates the information system that meets WHO’s goals. WHO has its Global tuberculosis control planned for the 2006-2015 period, when it aims to reduce TB global burden (incidence, prevalence and mortality). One of these goals regards reducing (in 50%the number of cases from 1990) its prevalence of and mortality cause by this disease in 2015[1]. It is very worth having reliable recorded notification data and patient monitoring, since incomplete TB patient data notification impairs patient’s location and it hinders the effectiveness of searching, assisting, treating and properly controlling the disease. Lack of information does not provide proper data of about the reality of Tubeculosis in the country.
Espírito Santo provides Health Care Units with supervised treatment since 2000 [4]. Data from the Brazilian National Disease Notification System (Sistema Nacional de Agravos Notificáveis – SINAN) show that 174 cases were reported in Serra County, in the State of Espírito Santo, in 2009; out of them, 169 live in the urban area [5].
The present research aims to study the importance of information records about TB patients assisted at CRA – Centro de Referência Ambulatorial (Brazilian Reference Ambulatory Center) [2].
The current study assessed 863 medical records of patients assisted at CRA in Serra County, from 2004 to 2009 and performed a descriptive analysis to find the statistical percentage of applied treatments. Semi-structured interviews with 12 social actors (members of the Tuberculosis Control Program in Serra) were conducted along with direct observations for qualitative data analysis; such data were analyzed by combining the research assumptions that aimed to follow the evaluation methods, the Social Programs Implementation [6] and the Logic Model Evaluation [7].
Development
Tuberculosis Control Policy in Brazil and the importance of information recording
The Brazilian National Health Council from August 6th- 1998, released resolution n. 284, due to the TB epidemiological calamity around world. The resolution took under consideration the reality of the disease in the country and concluded that the Emergency Plan – which is still under implementation – needed to be adjusted and expanded. The reality could and should be fixed if the available resources were used. It was decided that TB was a priority issue within public healthcare in Brazil and, according to the plan, the establishment of strategies to develop a new plan was suggested. Still, in 1998, the control of the National Coordination for Sanitary Pneumology (Coordenação Nacional de Pneumologia Sanitária – CNPS) returned to the Ministry of Health (MS – Ministério da Saúde) and it was linked to the Department of Health Policy (Secretaria de Políticas de Saúde – SPS). In October, 1998, the National Tuberculosis Control Program (NTCP) was launched and signed by the President of the National Health Council. The program followed general guidelines such as: a) MS is responsible for setting the rules; b) medicines acquiring and supplying; c) laboratory and treatment referencing; d) information system coordination; e) supporting states and counties f) intersectorial articulation to maximize public policy results. NTCP understands that it is mandatory to articulate complementary actions taken by social participation and non-governmental organizations in three National Health Care System “Sistema Único de Saúde –SUS” management levels (the Union, states and counties) [8-11].
Since 2003, fighting TB became a priority for the Federal Government. Patients’ care was decentralized and monitoring started to be done at primary care. More counties held the role of controlling the disease, as it was stated by NTCP’s coordinators [12].
The State of Espírito Santo recorded 1301 new TB cases in the Brazilian National Disease Notification System (Sistema Nacional de Agravos Notificáveis – SINAN) in 2004 and it represents 39.4 new cases in the state for each 100.000 inhabitants; 25.3 due to bacillus cases. The NTCP’s priority counties are: Viana, Guarapari, Cariacica, Vila Velha, Serra, Vitória, São Mateus e Cachoeiro de Itapemirim; however, the last two do not belong to the metropolitan area. The Directly Observed Treatment Strategy (DOTS) – known in Brazil as TS-DOTS – was implemented in 123 of the 1.097 state health units (11.2%).The cohort of treatment priority counties showed healing index of 82.5%, which is still below the target of 85%. The dropout rate was 5.1%; mortality, 7.1%; referring, 5.2%; and good closure rate in 95.3% of the cases. TB/HIV coinfection rate was 7.1% [13,14].
To reduce the number of TB and increase the percentage of diagnosis and cure, the Ministry of Health suggested investing R$119.5 million to reduce the number of TB cases and increase the percentage of diagnosis in 2007, as part of NTCP improvement. It represented the highest investment, in the last ten years, to fight the disease. One of the main problems to be faced is still the lack of information among the population. It is the major reason for the high tuberculosis rates in Brazil. For the very first time, the fight against Tuberculosis is among the 16 priority actions of the Ministry of Health [2]. Health Minister, José Gomes Temporão, states that investments in Tuberculosis prevention and control have increased 14 times, from 2002 to 2009. In 2002, the investment was of US$ 5.2 million. Between 2002 and 2009 it totaled US$ 74 million [12].
Data from SINAN show that in 2009, 174 cases were notified in Serra County (Espírito Santo State); 169 of them were recorded in the urban area [5].
Results
The current economic crisis had a strong influenced on the health system as TB patients come from low income classes and 90% of the population depends on SUS. There is a very strong influx at CRA Jardim Limoeiro; however, the Unit is not able to meet such demand. There was drop in revenues and on City Hall funds to health care. Hence, the payment of such funds was also affected. However, the county has received federal resources for the health programs and they could be used on equipment purchasing and on the opening of new health facilities, without spending more money with the construction of new Basic Health Units (Unidade Básica de Saúde-UBS”). The construction of these new units depends on Federal funds acquired through parliamentary amendments and on the agreement with the Emergency Care Units (Unidades de Pronto Atendimento-UPAs), which are also maintained by Federal funds.
Despite the current NTCP regulations, there are places in Brazil where TB treatment is still provided by specialized ambulatories rather than in expanded primary care networks. All the programs in the Southeast Region face the same difficulties, except for São Paulo, where TB services are not decentralized, but concentrated in only one health care center in each city. Thus, all the patients should go to a particular center to be assisted and to receive medication, transportation vouchers and food supplies. Besides, such service is not often close to the TB patients’ home and it does not befit NTCP recommendations – which bet on decentralization as the strategy to facilitate the access to disease diagnosis and treatment in a place closer to the patient’s residence (interviewee 1).
CRA is considered to be a sub-unit; however, it works as a basic unit. Out of all Serra’s UBSs, only three have TB control service: Boa Vista (Feu Rosa neighborhood), and CRA (Jardim Limoeiro). The county aims to implement prevention activities as well as TB case finding, diagnosing and treatment in every UBS; however, it has not been done.
Out of the 863 analyzed notifications, 11% were incomplete, as described in the table below.
The sum of deaths, dropouts, refers and incomplete notifications found in the analyzed records from 2004 to 2009 totaled 229 patients. When the number of uncured patients, from each of these years (229), is added to this total, the number jumps to 558 not controlled and assisted patients. This number represents 62.3% of the total of individuals who were affected and sought for TB service in CRA, as it can be seen in the graph below:
It is worth mentioning that in 2004 the TB cure rate in Serra reached 85% and it allowed stating that the county had reached the suggested MS goal for that year. CRA Jardim Limoeiro reached 82% disease cure. There was decrease in MS target, from 2005 to 2006. CRA presented 65% cure rate and this number decreased to 61% in 2006; however, it grew back in 2008 and 2009, and reached 83%. The index recorded between 2004 and 2009 represented 73% cure rate; 12% below that recommended by MS. The charts below show the above described data:
The following degrees of evaluation were adopted as reference points used to classify the number of incomplete notifications: excellent (less than 5%), good (5 to10%), regular (10 to 2%), bad (20 to 50%) and very bad (50% or more). It was found that CRA notification completeness was classified as regular, although it indicated improvement tendency.
TB control drop in Serra matches the decline in health investments in the county, according to the interviewees. The increase in the number of healed patients in 2009 is also directly linked to the new leap in investments that took place that year. So, despite the fact that public managers followed the same path and were in tune with the Secretary of State for Health and the State Government, when investments in health were reduced, the expected results in TB control sharply and quickly fell.
Authors corroborate the importance of investing financial resources to successfully TB eradication, since financial investment in the program targeting on prevention and disease control increased 14 times from 2002 to 2009, it went from US$ 5.2 million in 2002 to US$ 74 million in 2009 [12]. It is though stated that the close relation between administration and health public investment in the TB control programs is corroborated by the poor quality drugs, the frequent and prolonged shortage of antituberculosis drugs in health centers and the inadequate monitoring of patients by the health professionals and it is a strong risks to the effectiveness of the program [ 15-17]. Similarly, the political and social influence on TB control actions was identified [18].
By taking under consideration NTCP’s goal of properly treating100% of the TB cases, curing 85% of them and keeping dropouts within an acceptable level (up to 5%), it was found that CRA Serra showed cure rate decrease between 2004 and 2008 and significant improvement of it in 2009, when the county reached 83% of cure. Regarding the number of dropouts, it was found that the cure average throughout the studied period remained within the acceptable rates recommended by MS. However, when the year-to-year dropout rate was separately recommended, it was noticed increase from 3%, in 2004, to 9%, in 2009. According to the current study, it can be stated that the dropout rate remained low in 2004 and 2005 (Chart 4), but it considerably grew from 2006 to 2009; time when the number of dropout cases had risen from four to eleven (170%).
According to the interviewees, changes in the Municipal Government during the periods of 1997-2004, 2005-2008 and 2009-2012 did not lead to changes in patients’ care giving process; the process remained under the responsibility of the same program members. As the Municipal Secretary of Health remained the same, the team that was already working in the program remained practically the same and the members who were responsible for the program were officially hired by the local government. The political change did not affect NTCP implementation, although the county’s population had disorderly grown during the implementation period and the service did not follow its growth. The number of servers remained the same; the actions were municipalized and ended up holding the Health Department – which did not catch up with the population growth.
Conclusion
CRA presents poor structure in all aspects, from infrastructure – room size, poor ventilation, lack of proper medication storage, improper air filter positioning (which flows into the hallway, favoring disease transmission) – to human resources – inadequate number of professionals to cover the Program’s guidelines. The situation is hindered by the high turnover rate, which results from low salaries, infrastructure inadequacy and poor working conditions. Consequently, NTCP goals were not fully met by CRA. Inflexibility leads to consequent delay in action taking such as hiring professionals, decently wage paying, servers’ responsibility with patient care and the construction of rooms according to TB treatment recommendations.
Compulsory notification dues to the lack of structure in the City Health Department and in the UBSs. Some notifications are incomplete and may refer to inadequate perception of the county’s reality. Incompleteness index of the notified data is of approximately 10.5% and it allows classifying this index as regular, namely, the importance given to information recording is insufficient if one considers that it is a contagious infectious disease and that its control ensures policies’ positive results. The same results depend on relevant accurate information from each patient and on routine suitability in each service.
It is worth explaining that the multidisciplinary team, the technicians’ team and the graduated team are staff outsourcing. The social workers should be better trained in order to perform more appropriate approach to ensure the patients’ right of being individually monitored.
The situation of those who work with infectious disease is, therefore, a political issue which needs to be urgently revised. There is lack of professionals willing to work in the program due to low wages, job insecurity and to the no additional payment of unhealthy work.
The poor working conditions, the non-availability of protective material and the lack of information among professionals regarding the need of using such material are some of the factors observed in the study held in Vitória, Espírito Santo State [19].
The training of professionals working in TB control and prevention and the development of educational health actions as well as of communication and social mobilization practically do not exist, although it is recommended by MS. As staff turnover is high, a lot of information is lost and it stops greater professional involvement with the importance of controlling the disease.
________________________________________
[1] The year of 2000 showed 48.4 / 100.000 inhabitant incidence and it means 82.249 new TB, mortality coefficient 3.7 / 100.000 inhabitants (BRAZIL, 2004); in 2005, an evaluation held by the World Health Organization (WHO) indicated that among the 22 countries with the highest TB levels in the world, the cure rate of this disease in Brazil (81%) was the ninth worst one.
[2] the study was recorded and approved under n. 006/2010 at the School of Sciences Research Ethics Committee of Santa Casa de Misericordia, Vitória, EMESCAM. ________________________________________
References
- OMS- Organização Mundial de Saúde. Global tuberculosis control:Surveillance, Planning, Financing. Geneva, World Health Organization, 2007.
- Brasil. Ministério da Saúde. Sistema de informação de agravos de notificação. Área técnica de pneumologia sanitária. Brasília, 2004.
- Ministério Da Saúde. Secretaria de Políticas de Saúde do Departamento de atenção básica. Caderno de atenção básica, n. 6, Brasília: Ministério da Saúde, 2002. Dispõem sobre o Manual técnico para o controle da tuberculose.
- Ministério Da Saúde. Plano nacional de mobilização e intensificação das ações para a eliminação da hanseníase e controle da tuberculose. Brasília, 2001.
- Ministério Da Saúde/SVS- Sistema de Informação de Agravos de Notificação (SINAN e base populacional IBGE, 2009. Disponível em: Acesso em 19 julh. 2009.
- Draibe S M. Avaliação da implementação. Esboço de uma metodologia de trabalho em políticas públicas. In: BARREIRA, M. C. R. N; CARVALHO, M. C. B.(org.). Tendências e perspectivas na avaliação de políticas e programas sociais. São Paulo: IEE/PUC-SP, 2001.
- Yin R K. Estudo de Caso: Planejamento e métodos. Trad. Daniels Grassi. 3.ed. Porto Alegre: Brookman, 2005.
- Ruffino-Netto. Tuberculose: a calamidade negligenciada. Rev Soc Bras Med Trop. 2002; .35(1): 51-8
- Ministério Da Saúde. Secretaria De Vigilância Em Saúde. Departamento De Vigilância Epidemiológica. Programa Nacional De Controle Da Tuberculose. Nota técnica sobre as mudanças no tratamento da tuberculose no Brasil para adultos e adolescentes. Brasília; 2009[citado 2009 dez 10]. Disponível em: Acesso em: 11 out. 2010.
- Ruffino- Netto, A. Impacto da Reforma do setor de saúde sobre os serviços de tuberculose no Brasil. Bol Pneumol Sanit. 1999, v.7, n. 1,.
- Conselho Nacional De Saúde. Resolução nº 284 de 06/08/98 do Conselho Nacional de Saúde-Dispõe sobre o Plano Nacional de Controle da Tuberculose .Brasília, DF, 1999.
- Barreira, D. Brasil reduz incidência da tuberculose e melhora posição na lista dos países com maior número de casos no mundo. Imprensa livre, Ubatuba, 13, mar. 2010. Disponível em:
- Ministério Da Saúde- Relatório da situação – Espírito Santo, Sistema Nacional de vigilância em saúde. 2, ed. Brasília, 2006.
- Moreira, C. M. M. Maciel, E. L. N. Completude dos dados do Programa de Controle da Tuberculose no Sistema de Informação de Agravos de Notificação no Estado do Espírito Santo, Brasil: uma análise do período de 2001 a 2005. J Bras Pneumol. 2008;34( 4): 225-9.
- OMS- Organização Mundial de Saúde. Directrices para el tratamiento de la tuberculosis farmacorresistente. WHO, Geneva, 1997.
- Pfyffer, G. E. Drug-Resistant Tuberculosis: Resistance Mechanisms and Rapid Susceptibility Testing. Schweiz Med Wochenschr. 2000; 130 p. 1909-1913.
- Paramasivan, C. N.; Venkataraman, P. Drug Resistance In Tuberculosis In India. Indian J Med Res.2004; 120: 377-386.
- Mishima, E. D.; Nogueira, P. A. Tuberculose no Idoso: Estado de São Paulo, 1940-1995. Bol Pneumol Sanit. 2001: 9(1): 5-11.
- Prado T.N., et al. Perfil epidemiológico dos casos notificados de tuberculose entre os profissionais de saúde no Hospital Universitário de Vitória (ES) Brasil. J Bras Pneumol. 2008;34(8): 607-613.
Attachments
Table 1: Absolute and percentage numbers of TB patients treated at the CRA Serra-ES, according to final classification and period (2004-2009).
| Year | N. º Tb | Healing | Deaths | Transfers | Abandonment | Incomplete Reports |
| 2004 | 189 | 155 (82%) | 11 (6%) | 7 (4%) | 6 (3%) | 10 (5%) |
| 2005 | 149 | 97 (65%) | 9 (6%) | 8 (5%) | 4 (3%) | 31 (21%) |
| 2006 | 148 | 91 (61%) | 3 (2%) | 10 (7%) | 7 (5%) | 37 (25%) |
| 2007 | 117 | 76 (65%) | 8 (7%) | 9 (8%) | 10 (9%) | 14 (12%) |
| 2008 | 143 | 118 (83%) | 3 (2%) | 12 (8%) | 9 (6%) | 1 (1%) |
| 2009 | 117 | 97 (83%) | 2 (2%) | 6 (5%) | 11 (9%) | 1 (1%) |
| TOTAL | 863 | 634 (73%) | 36 (4%) | 52 (6%) | 47 (5%) | 94 (11%) |
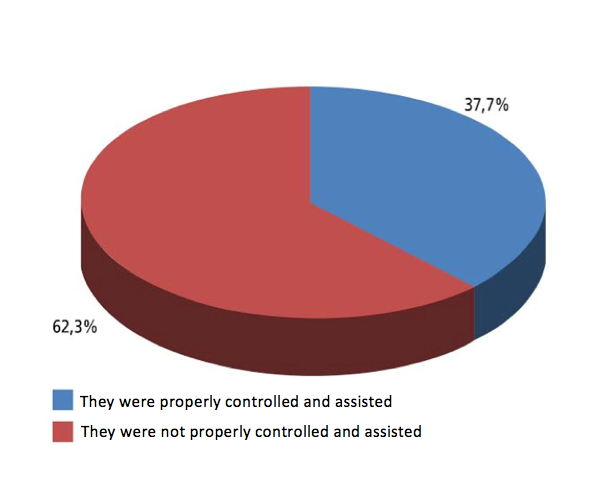
Figure 1: Percentage of patients with TB on a demand for the service in 2004-2009. CRA Serra-ES.
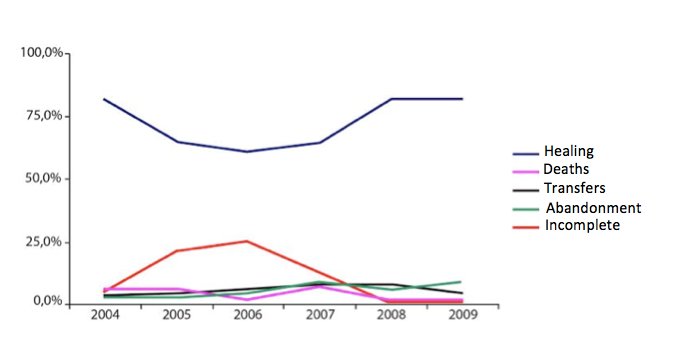
Figure 2: Relationship between the percentage of healing, deaths, transfers, abandonment and incomplete notifications per year. CRA Serra-ES (2004-2009)
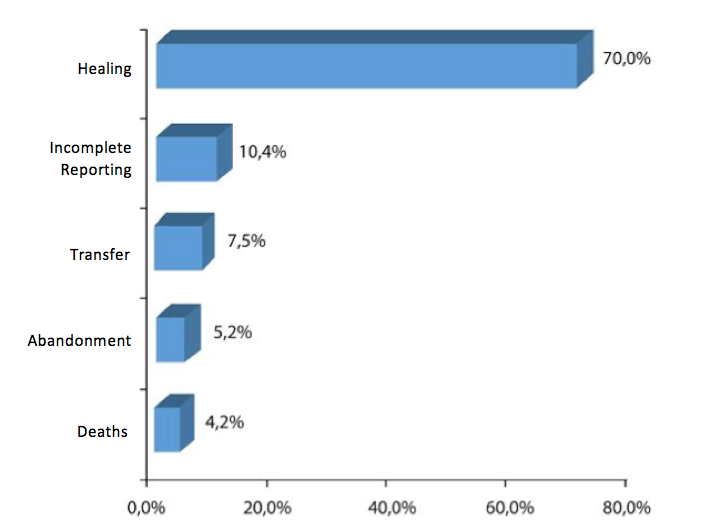
Figure 3: Percentages of healing, incomplete notifications, transfers, abandonment and deaths in the CRA Serra-ES (2004-2009).
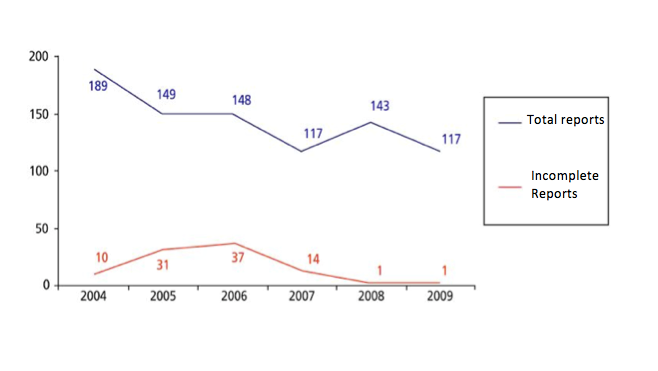
Figure 4: Evolution in the number of incomplete notifications according to the year in the period 2004-2005 – CRA Serra-ES.
Authors
Mariangela Braga Pereira Nielsen: Master/ EMESCAM – (teacher).
Alacir Ramos Silva: Doctor/UNB – (Researcher do Locusss/UNB ; de Harvard Medical School, – USA , de MèdicnesSans Frontieres e do Violence Reseacher’s Consortiunm – France ).
